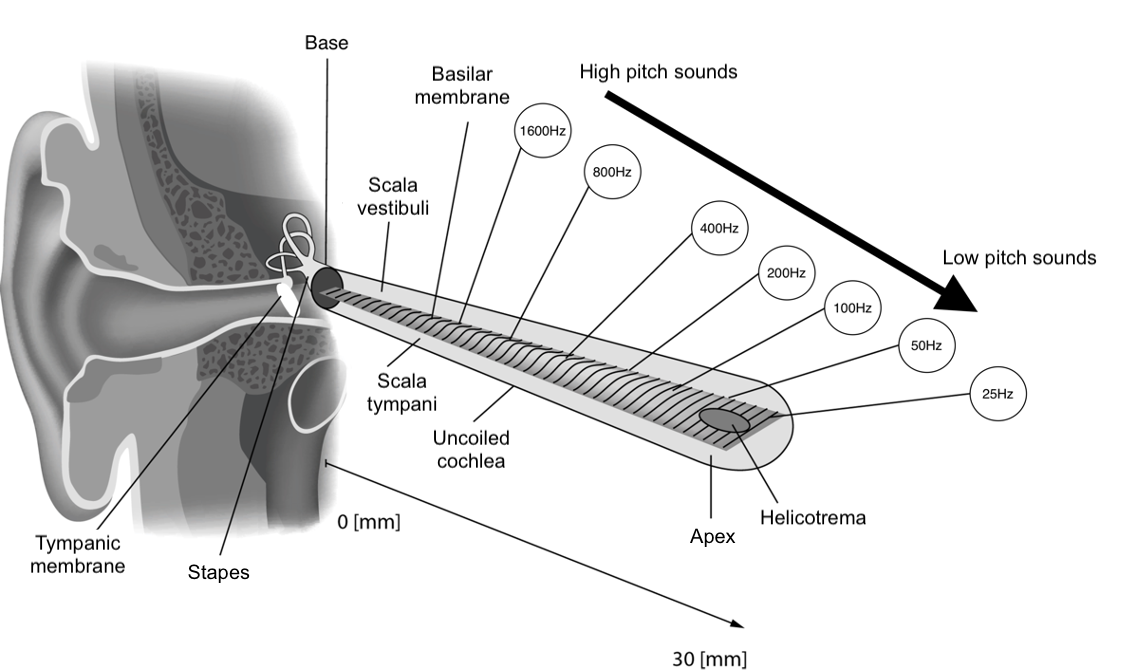
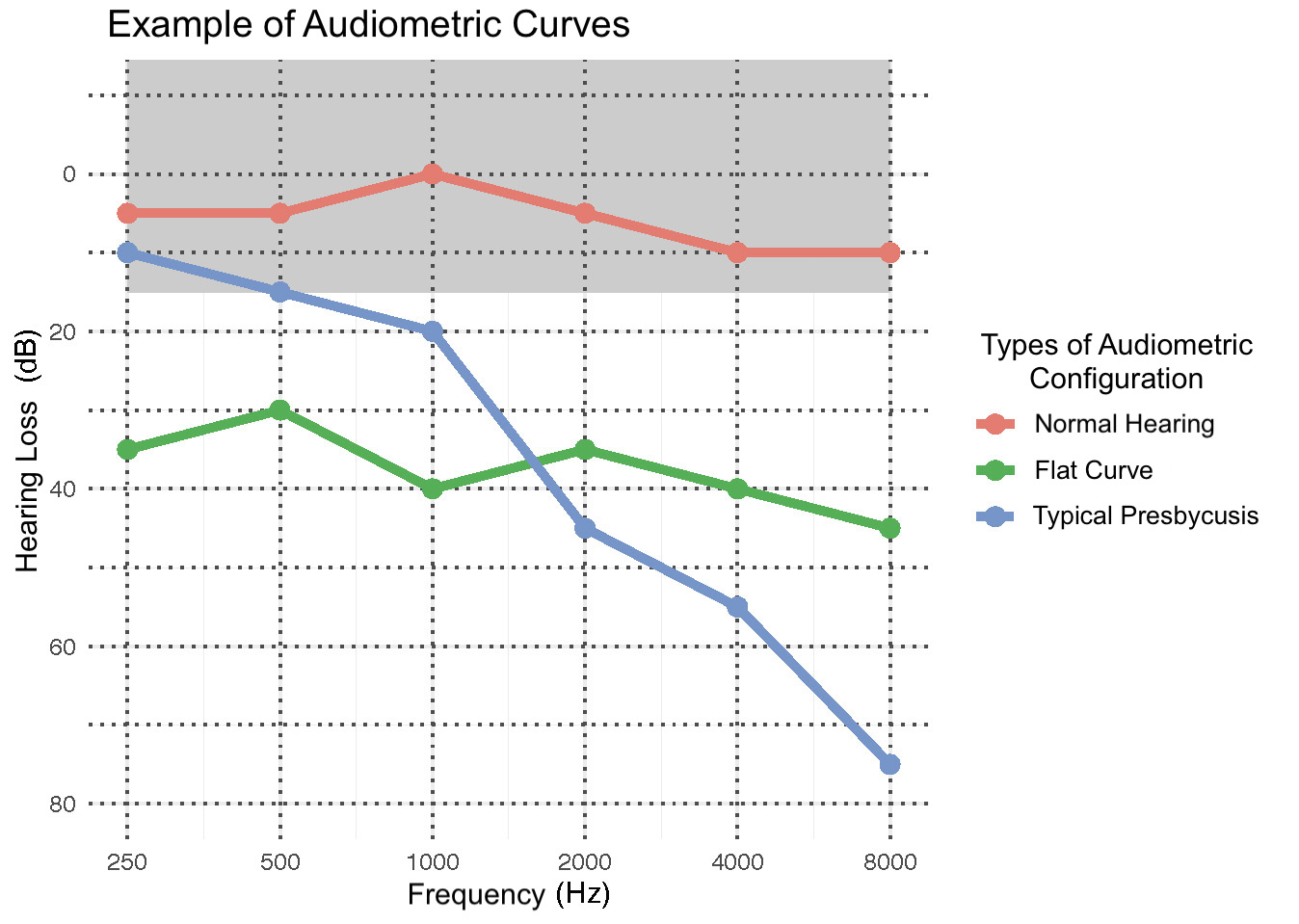
The different types of presbycusis presented in this section are based on studies conducted using cell samples taken from deceased individuals for whom audiograms were available (Figure 5). By comparing the cellular samples with the audiometric curves of these individuals, research teams were able to determine the impact of various cochlear impairments on auditory acuity as measured by audiometric evaluation.
Sensory Presbycusis
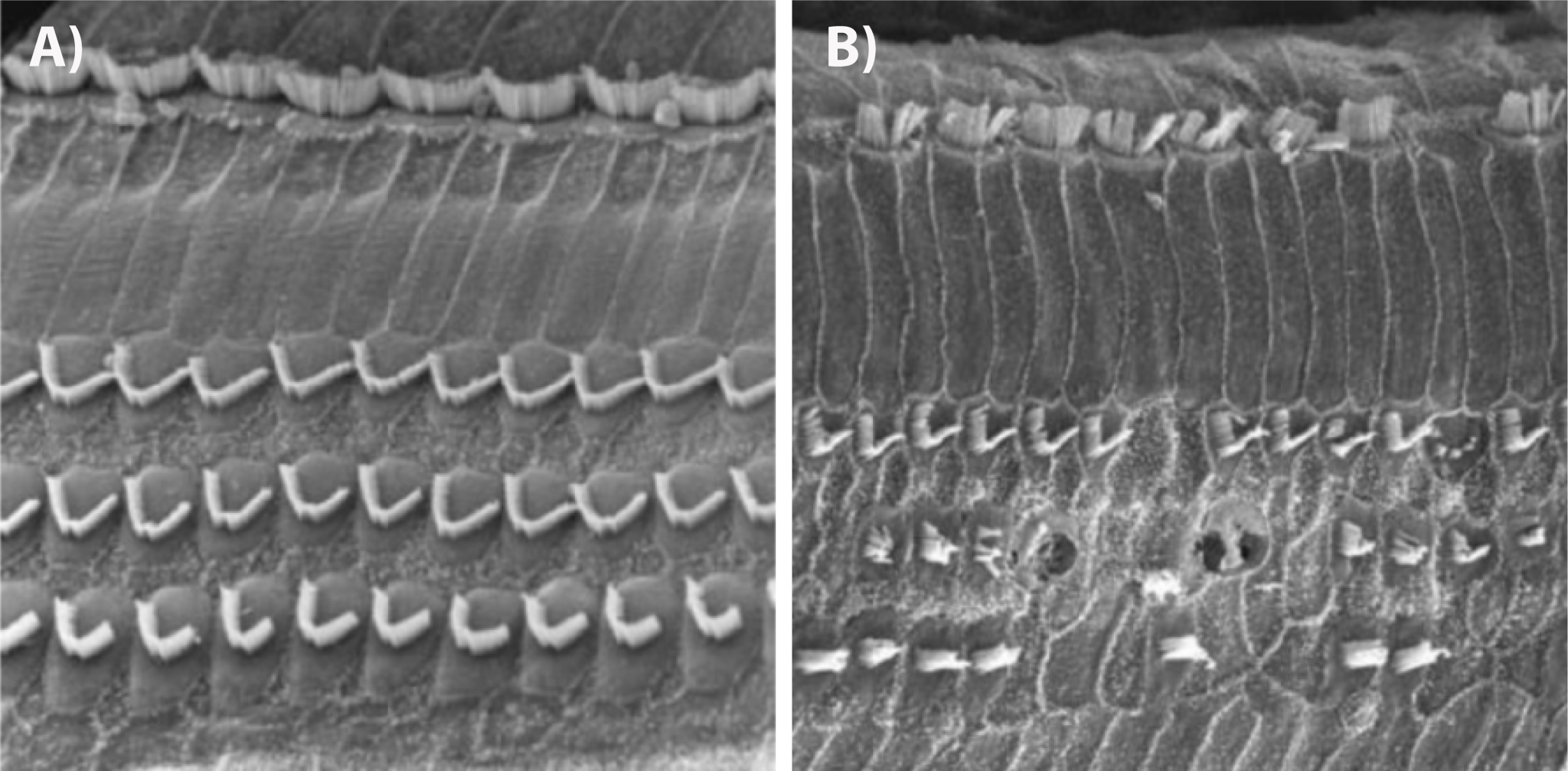
This form of presbycusis is characterized by the loss of outer hair cells at the base of the cochlea (approximately 0 to 12 millimeters). In more advanced stages, atrophy of the supporting cells of the organ of Corti can be observed. This loss results in a deficit in the perception of high-pitched sounds, but it rarely affects auditory acuity to the point of causing serious speech perception difficulties that are hard to compensate for with hearing aids (Figure 5, blue curve). This type of presbycusis is thought to be partly hereditary in both men and women. Cumulative noise exposure over a lifetime is the most significant contributing factor to this type of presbycusis, which is also considered the most common.
Neural Presbycusis (sometimes referred to as Central Presbycusis)
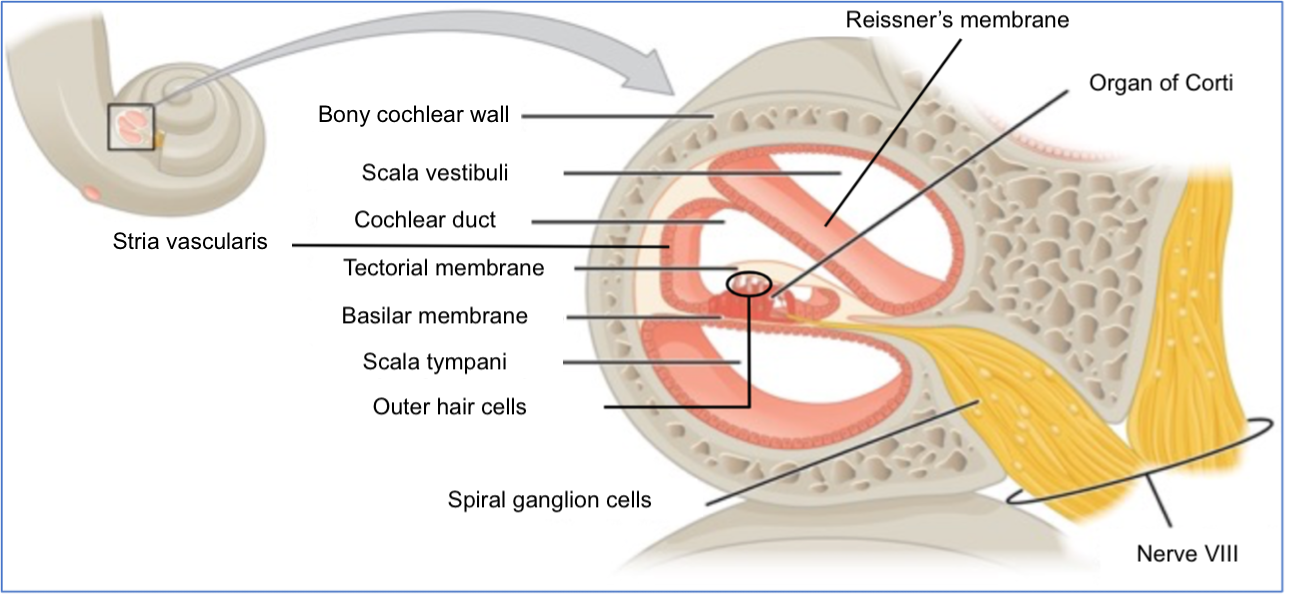
This type of presbycusis is defined by the loss of ganglion cells in the spiral ganglia (Figure 4). The loss of these cells can result in varying degrees of hearing loss depending on the location of the affected cells. Ganglion cell loss can occur along the entire length of the cochlea. This type of presbycusis is primarily manifested by speech perception difficulties that are more significant than the individual’s audiometric curve would suggest. Indeed, 75% of spiral ganglia can be affected without impacting auditory acuity as measured by pure-tone audiometry. The effects of this type of presbycusis generally become apparent in advanced age when the number of ganglion cells falls below a critical threshold. This presbycusis is more challenging to compensate for with hearing aids, especially when ganglion cell loss is more significant in the cochlear regions crucial for speech perception.
Metabolic Presbycusis (sometimes referred to as Strial Presbycusis)
This type of presbycusis is characterized by insufficient blood supply to the stria vascularis, leading to a chemical imbalance in the endolymph, which is necessary for proper hair cell function. Metabolic presbycusis is associated with a reduction in low-frequency hearing acuity because it affects the stria vascularis along the entire length of the cochlea (Figure 5, green curve). This type of presbycusis is most strongly associated with aging. It has a stronger hereditary component than sensory presbycusis and is more prevalent in women. Cardiovascular diseases are a significant contributing factor, particularly in women.
Mechanical Presbycusis
Mechanical presbycusis is thought to be associated with the stiffening of the basilar membrane and consequently the organ of Corti. This type of presbycusis is associated with when people presenting with a typical audiometric curve showing high-frequency loss, and no signs associated with other types of presbycusis. Some authors suggest that this pathophysiological mechanism is theoretical since there is very little evidence and scientific explanation for the phenomenon of basilar membrane stiffening. Additionally, the literature remains unclear about the precise manifestations of this type of presbycusis on the auditory acuity of those affected.
Mixed Presbycusis
Mixed presbycusis occurs when at least two of the characteristic traits of the aforementioned types of presbycusis are present (loss of hair cells at the base of the cochlea — loss of ganglion cells — dysfunction of the stria vascularis — stiffening of the basilar membrane). This form of presbycusis can therefore result in a wide variety of configurations, hearing losses, and specific difficulties associated with them.
Intermediate Presbycusis
This type of presbycusis involves submicroscopic alterations in intracellular organelles, dysfunctional cellular metabolism, a decrease in the number of synapses on hair cells, and chemical alterations in the endolymph. The audiometric curve associated with this type of presbycusis is relatively flat across all frequencies, with a slightly more pronounced drop in high frequencies. It could correspond to the green curve in Figure 5.

{kind=link}