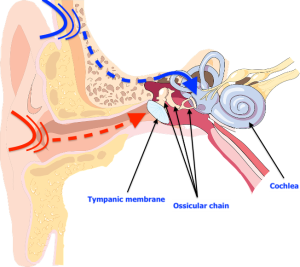
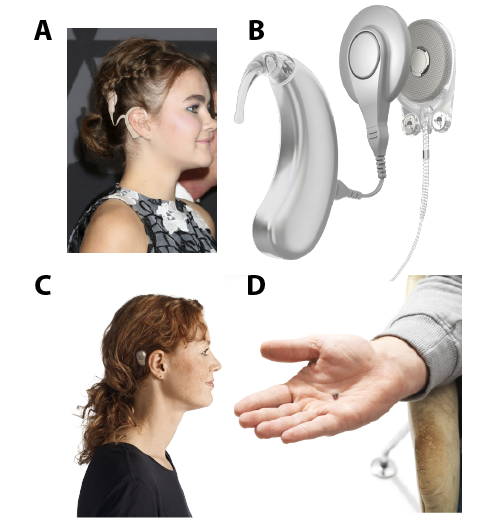
Audiology and the work of audiologists











Address
2301 Av. D'Estimauville,
Quebec, Qc G1E 1T2
Emaillaboratoireparole@crulrg.ulaval.ca
Call Us418-821-1229


{kind=link}